


Introduction
She is a 12-year-old who needs to stay in school, be adequately nourished, learn how to keep herself safe and healthy, and be vaccinated against HPV to protect her from cervical cancer later in life. She is a single 16-year-old who seeks to complete her secondary education and find a job, while meeting her needs for voluntary contraceptive choices and protection against HIV. She is a married 24-year-old who wants to provide for her family, control the timing and spacing of her pregnancies, survive childbirth, live a healthy full life, and have strong, well-nourished children.
As the adolescent girl becomes a young woman, her life prospects and those of her children will rest on access to several vital interventions that are commonplace in the United States: information and services on voluntary contraceptive choices, access to education and prevention of early child marriage, basic nutrition, vaccines to prevent cervical cancer, economic opportunities, and reliable protections against violence. How her life evolves will rely on access to quality care, informed decisions, and critical support structures.
We have a historic opportunity to make a difference—for her future, for the future of her family and community, and for our own—by providing the tools that allow her to realize her full potential.
From our co-chairs
“The work of the CSIS Task Force exemplifies how people with different perspectives can unite behind a common mission and work to create positive change. We were fortunate to have the insights of leaders from Congress, industry, foundations, universities, the faith community, and nongovernmental organizations, among others, all committed to building on the impressive American legacy in global public health. The resulting vision of improving the health and well-being of adolescent girls and young women, and in doing so, unleashing their economic and social potential, will resonate throughout our society and can be realized with the determined leadership of both Congress and the administration.” — Helene Gayle
“As a global health leader, the United States has a unique ability to help improve the lives of girls and women in developing nations. Through the partnership of government, businesses, and nonprofits, and by leveraging the innovation and technology that America is known for, together, we can truly help change lives in a powerful and lasting way.”— John Hammergren

Photo credit: Sala Lewis
Recommendation
The CSIS Task Force recommends that the Trump administration, in concert with Congress, launch a signature health initiative that targets not a single disease or global health challenge, but rather an important population: adolescent girls and young women (ages 10–24).
The Goal: To secure the health and future of adolescent girls and young women in 13 low-income countries. Doing so will generate vital returns over the course of their lives and the lives of their children, significantly strengthening families, communities, and societies at-large.
The Strategy: Concerted U.S. high-level
leadership over the next four years will expand proven
interventions that advance maternal and newborn health,
family planning and reproductive health, nutrition, and
prevention of cervical cancer. It will build upon the
PEPFAR structures that have achieved dramatic gains in
reducing the risk of HIV infection. Success will be aided
by a tight geographic focus on 13 target countries, and a
careful, systematic approach that joins the expansion of
health-related services with improved access to education,
economic empowerment, and gender-based violence prevention
and response programs. The strategy will rely on
innovative approaches to technology, lessons learned from
the business community, systematic use of existing
investments, strong governance and accountability,
engagement of men and boys, and aggressive mobilization of
diverse financial resources, including expanded
contributions by the private sector.

Photo credit: Sala Lewis
The Rationale
Why this population now?
A Period of Immense Change for Young Women: Early adolescence (10 to 14 years) is a critical time to build on previous investments in child health, nutrition, HIV prevention, and education, and to lay the foundation for continued cognitive and physical development. The onset of puberty is an important time to reach girls with information about reproductive health, nutrition, gender-based violence, and gender equality.
Late adolescence (15 to 19 years) represents an important period to build and expand health and education gains. In the developing world, the average adolescent girl often becomes sexually active, marries, and has her first child in this period—one of many reasons why only 18 percent of young women complete secondary school across the 13 target countries.
Young adulthood (20 to 24 years) is a critical time for young women to sustain health gains and realize their full earning potential. In developing countries, many young mothers quickly become pregnant again, which increases the risks for mother and newborn of dying during childbirth, as well as illness and other complications during and after delivery. It also decreases their access to social and economic opportunities.
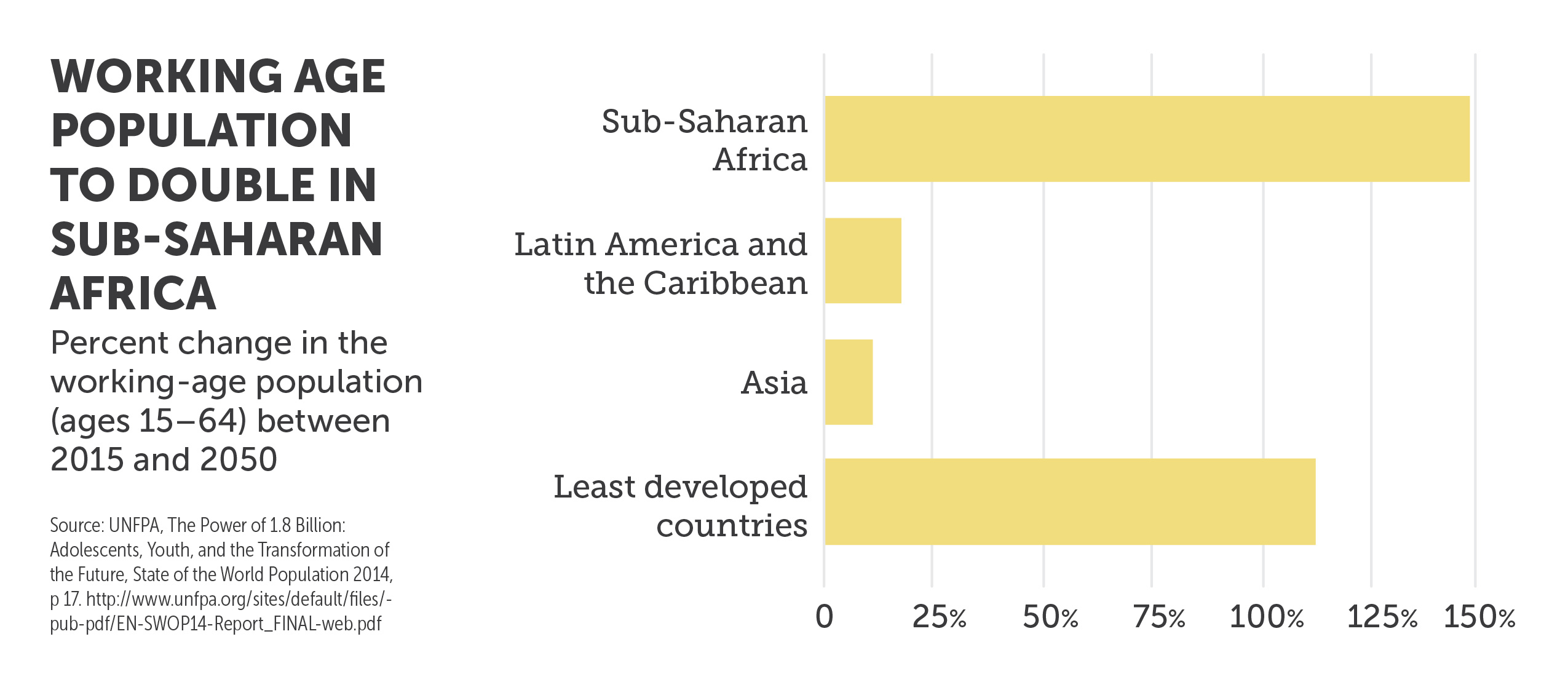
An Urgent Need: The adolescent and young adult population in low-income countries is at a historic high and will continue to rise in the coming years.1 This demographic phenomenon, a central dimension of the “youth bulge,” threatens to lead to high unemployment and instability, including in countries that matter significantly to U.S. national interests.2 Recent progress in reducing deaths among children under the age of five means there are more young women than ever in history who need to be reached with critical services. As these young women navigate the journey between childhood and adulthood, they and any children they bear face perilous health risks that can both compromise their potential and impose grave costs to society.
Too often, adolescent girls and young women, especially those living in poverty, fall through the cracks: they live with high risks of early marriage, unintended pregnancy, gender-based violence, and exploitation, which in turn leave them at high risk of maternal mortality and serious illness, birth complications, HIV infection, and cervical cancer. Within the household, they are often the last to eat, putting them at increased risk of malnutrition. As these risks intensify, lifetime educational and economic opportunities slip away.3
A High-Yield Opportunity. Investing in adolescent girls and young women, we now know, has a triple impact:
- On the lifetime of that individual;
- On the lifetime of her children, the next generation; and
- On the broader prosperity of her community.4
According to the World Bank, improving health outcomes for women can increase labor productivity by as much as 25 percent in some countries.5 By supporting young women today and assisting them to become productive members of society tomorrow, the world economy stands to grow by as much as $12 trillion, should women be permitted to play an equal role in labor markets as men.6 Achieving a fraction of that increase through these interventions will help to improve economic outcomes in the 13 target countries.
Major Global Health Initiatives
A Chance to Make History: The Sustainable Development Goals (SDGs), The Lancet commission on adolescent health and wellbeing, Family Planning 2020, and the UN Secretary General’s Global Strategy for Women’s, Children’s and Adolescent’s Health have generated considerable global momentum in support of adolescent girls. U.S. policy has recently added a significant new dimension with the launch of the landmark, ambitious PEPFAR DREAMS partnership, which concentrates efforts to reduce the extreme risks of HIV infection faced by adolescent girls and young women in “hot spots” in 10 sub- Saharan African countries. Other related U.S. policy efforts include the Let Girls Learn initiative, the Global Strategy to Empower Adolescent Girls, and the USAID goal of ending preventable child and maternal deaths. Meanwhile, important public-private partnerships such as Saving Mothers, Giving Life have demonstrated the possibility of achieving concrete gains in reducing maternal mortality,7 while Pink Ribbon Red Ribbon has done the same for preventing and treating cervical cancer.8
What is missing today is a viable, integrated plan to meet the unique needs of adolescent girls and young women that has substantial financial backing from diverse sources and can deliver concrete gains in health and educational and economic prospects. Making better use of data and surveillance tools will allow us to target services where they are most needed. This is what the proposed U.S. signature initiative seeks to achieve under the Trump administration.
The Action Plan
“The United States has the requisite institutional capacity, leadership, and economic resources to lead a high-yield global health initiative that would spur economic and social development. Our proposal highlights the scale and urgency of the challenge and lays out a strategic guide path for achieving an ambitious set of health care goals for young women.” — Ezekiel Emanuel
1. Focus on 13 target countries.
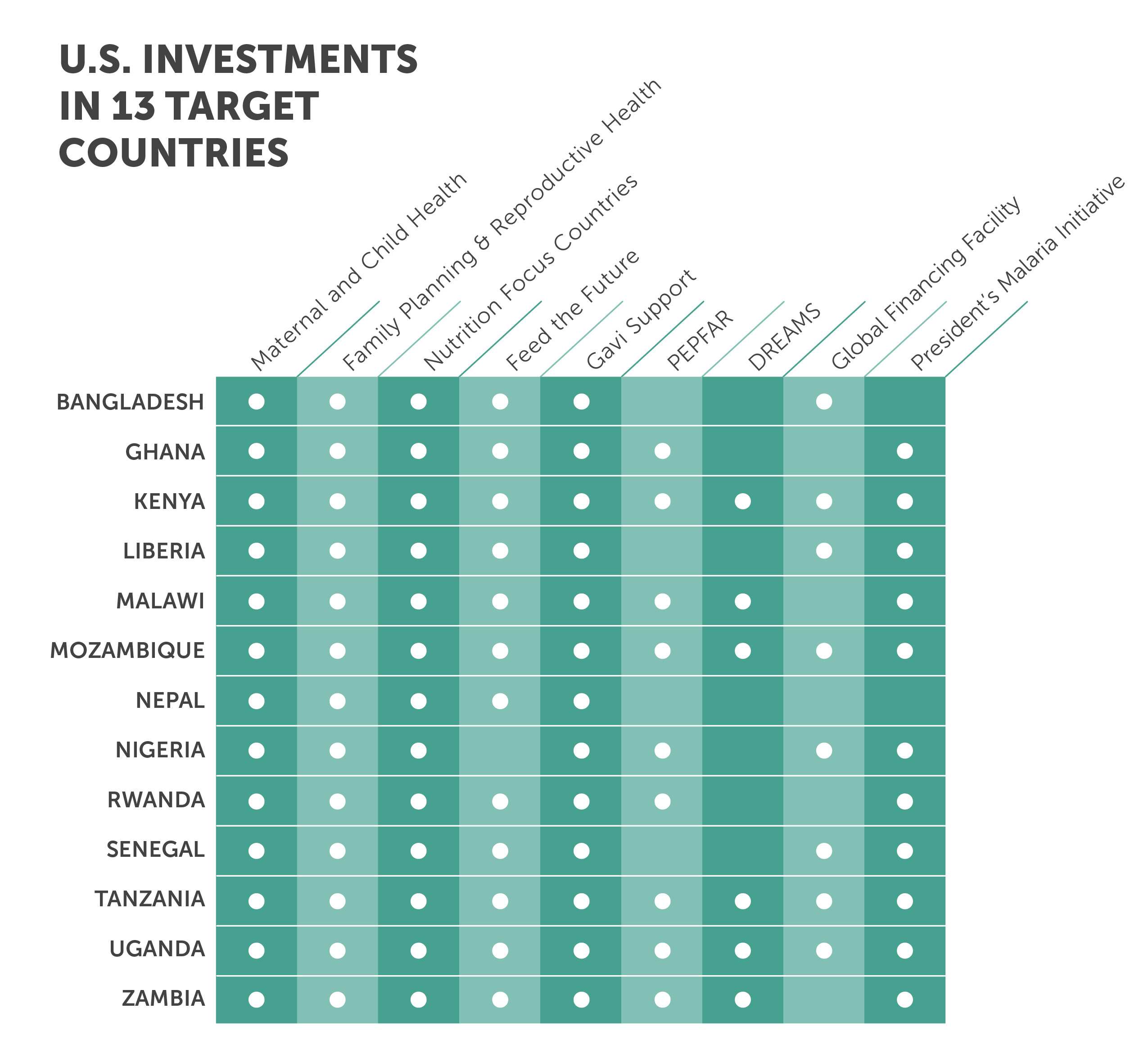
The initiative will focus on adolescent girls and young women in 13 low-income countries with great needs and substantial existing U.S. investments in health and related development areas, through both direct bilateral programs and multilateral agencies. The suggested target countries include Bangladesh, Ghana, Kenya, Liberia, Malawi, Mozambique, Nepal, Nigeria, Rwanda, Senegal, Tanzania, Uganda, and Zambia.9 Given the large populations of Nigeria and Bangladesh, we propose an initial effort to reach 20 percent of adolescent girls and young women in these two countries.
2. Build on existing U.S. investments.
The target population is diverse and includes sub-cohorts (e.g., in- and out-of-school, married and unmarried, pre- sexual debut and sexually active). Engaging with this group requires an approach that spans health and non-health sectors and special care in oversight, coordination, and delivery. Health providers will need to be trained and supervised to provide this population with quality and respectful care.10 Adolescent girls and young women and their communities will need to play an active role in the design and execution of programs.
The proposed approach takes full advantage of global health and related development investments in each country to target the special needs of adolescent girls and young women. That means systematically leveraging the DREAMS partnership (active in six of the target countries); its platforms offer exceptional opportunities for incorporating the initiative’s core health and development activities. It means tapping existing health investments in family planning and reproductive health; maternal, newborn, and child health; immunizations; and nutrition. It means taking full advantage of PEPFAR’s major capacities; investments in primary and secondary education; evolving work in food security; and programs to strengthen women’s empowerment, address gender-based violence, and prevent child marriage.
3. Spearhead new, ambitious goals in four key areas
- Maternal and newborn health: Increase by 25 percent the proportion of adolescent girls accessing high-quality care (antenatal, intrapartum, and postpartum) to address the health and social risks associated with adolescent pregnancy and childbirth, and improve newborn outcomes.
- Family planning: Increase access to voluntary family planning with the goal of meeting 50 percent of the current unmet need for modern methods of family planning among 15- to 24-year-olds who desire to avoid, space, or delay pregnancy. Girls between the ages of 10 and 14 require information and education to build their awareness.
- Nutrition: Reduce anemia by 25 percent among adolescent girls and young women by providing iron and folic acid supplementation, as well as nutrition education and counseling, to at least 75 percent of 10- to 24-year-olds.
- Vaccination against HPV: Prevent cervical cancer by achieving 50–75 percent coverage of HPV vaccine among 9- to 14-year-old girls. This effort would seek to fully immunize 40 million girls.
Click here to download chapter.
Click here to download chapter.
Click here to download chapter.
Summary of Health Impacts of Proposed Initiative
- Maternal and newborn health: 26,300 maternal and 493,000 newborn deaths averted.
- Family planning: 5.4 million users reached, 1.3 million unintended pregnancies averted, and 3,600 maternal deaths averted.
- Nutrition:25 percent reduction in anemia among adolescent girls and young women, contributing to the global goal of 265 million fewer women with anemia and 800,000 child deaths averted.
- Vaccination against HPV: 235,000 lives saved and 650,000 cases of cervical cancer averted.
Each of these efforts addresses an area of acute, unmet need. Each creates a bridge to this difficult-to-reach population. Each builds on mounting international and country-level action, accumulating evidence, and programmatic knowledge.
The four efforts reinforce one another. Improved access to family planning, for instance, assists in averting teenage pregnancy, which also helps maintain a girl’s physical and cognitive growth and lowers the odds she will die while giving birth.11 The introduction of HPV vaccines creates an opportunity to reach adolescent girls with additional sexual and reproductive education to further reduce the risks of early pregnancy and sexually transmitted infections (STIs).12 An investment in one area can stimulate investment in the others, while a platform designed for one program can potentially be used to advance the others.

Photo credit: Caitlin Healy
4. Align U.S. government leadership and oversight.
- The secretary of state should be responsible for the initiative’s overall strategic design and direction, including both shaping the U.S. budgetary process in Washington, D.C. and winning greater ownership by partner governments: e.g., encouraging legal and policy changes, along with higher budgetary commitments. The secretary should designate a deputy to track developments and convene an interagency steering committee comprising the executive branch departments and agencies with programs targeting adolescent girls and young women.
-
USAID: Operations and programmatic
decisionmaking need to be centered at USAID, which
implements most health, education, economic
strengthening, and agriculture programs that impact
adolescent girls and young women. A senior figure—the
equivalent of a deputy administrator—should be charged
with day-to-day leadership and management, including
developing strategies, budgetary allocations, staffing,
monitoring and evaluation, support to missions,
testimony before Congress, liaison to the White House,
and quarterly and annual reporting.
The USAID deputy administrator and the secretary of state’s designated deputy should share responsibility for relations with Congress and coordination of high-level diplomacy with host governments, U.S. corporate leadership, foundations, and international and multilateral organizations, and other donors. - U.S. missions:In each of the 13 target countries, the chief of mission should be responsible for political leadership in-country and management of relations with the host government, including all formal collaborations with partner governments. A senior coordinator should be responsible for day-to-day in-country management and coordination across U.S. government programs.
5. Sustain high-level diplomacy.
Led by the secretary of state, the United States has to think a decade or more into the future, while putting in place adequate metrics; insisting upon innovation; bringing to scale partnerships with governments, the private sector, multilateral institutions, civil society, and others that are both dynamic and catalytic; and systematically building coalitions committed to meeting the needs of adolescent girls and young women. Success will take time and requires strong, resilient, and innovative partnerships and approaches.
Diplomacy will be integral to encouraging partner governments to adopt policies that address the needs of adolescent girls and young women and invest at high levels in new partnerships. Diplomacy can shape markets to lower product costs and influence political and business decisionmaking. It can encourage businesses to invest in health services and in research and development (R&D) of appropriate technologies. It can also enlist civil society groups and faith-based organizations, foundations, international organizations, and other donors into the initiative.

Photo credit: Rick Bloom
6. Put innovation at the center.
- Invest in data. America leads the way in innovation, but that power is currently underleveraged in global health programs. A special effort is needed to better target and track unreached adolescent girls and young women and increase the impact of programs. In order for these proposed health interventions to succeed, better information is needed: e.g. data disaggregated by sex, age, marital status, and economic standing. Deeper knowledge is also needed in a number of key areas: e.g., how best to address gender-based violence, change norms around harmful practices such as early marriage, and how best to engage boys and men.13 This requires a significant investment in research to accelerate development of standard indicators and understanding of adolescent health outputs and outcomes. We are at a moment where these tools are becoming more available.
-
Spur research and development. Many
promising technologies and innovative approaches can
have major impact, specific to the needs of adolescent
girls and young women, in maternal and newborn health,
family planning, nutrition, and HPV vaccines.14
Digital health solutions, such as handheld devices and
electronic reporting systems, have the potential to
address the needs of adolescent girls and young women
and significantly improve their health outcomes in
low-resource settings. Many of these solutions will be
generated through partnerships with the private
sector.
To speed products from development to delivery, the secretary of state should create a high-level expert panel to advise on technological opportunities and public-private partnerships. USAID should create a dedicated mechanism to provide finances and technical expertise to emerging innovators in the 13 target countries. - Incentivize integration. In their country planning, U.S. missions should be systematically incentivized to combine programs in education, economic empowerment, gender-based violence, food security and reducing child marriage with their core health interventions, along with the operational research described above. An Integration Fund should be established at USAID that supports creative program alignments through results-based financing, founded on the outstanding quality of country plans that seek to demonstrate progress in achieving higher cost effectiveness and improved health outcomes.
-
Expand the role of the private sector.
The U.S. country teams in the 13 target countries should
partner with the local private health sector to expand
access to high-quality family planning and maternal
health services to adolescent girls and young women. The
U.S. should draw on the private sector’s expertise,
investment capacity, and special knowledge of local
customs and market conditions.
The Trump administration and Congress should support legislative action that authorizes and funds matching resources for public-private partnerships, including through innovative financing mechanisms15 that work to meet the specific needs of adolescent girls and young women.16
“Clearing the barriers that keep adolescent girls and young women from reaching their full potential cannot be addressed by one sector alone. Developing smart, multisectoral partnerships will give us the greatest chance to achieve our bold ambitions to improve the lives of adolescent girls and young women around the world.” — Christopher Elias
7. Mobilize robust financing from multiple sources.
The aggregate, new additional cost of the proposed initiative for adolescent girls and young women is approximately $634 million, comprised of the estimated annual cost of $176 million for maternal and newborn health, $144 million for family planning and reproductive health, $22 million for nutrition and nutrition-focused research, and $105 million for vaccination against HPV. It also includes $15 million for data and metrics, $25 million for innovation, and $100 million per year to add additional programs such as education, reward outstanding integrated country plans, and advance operational research, all financed through a results-based approach. Detailed cost analyses for each of these efforts follow this synopsis.
“Promoting the health of women and girls is one of the most effective ways to save lives and protect families in developing countries. If we succeed, it would also lead to more stable societies and improve our own national security, which are goals shared by Republicans and Democrats alike. As we continue to work with the private sector, nonprofits, the faith community, partner countries, and others in implementing this proposal, it is my hope that this bipartisan proposal will be embraced by policymakers on both sides of the aisle.” — Sen. Susan Collins (R-ME)
To be effective, the initiative will need guaranteed resources for at least the duration of the new administration, 2017 through 2021, with the expectation that funding will extend through 2025.
There are different options for phasing this initiative and for bringing adequate resources to bear. The Trump administration, in concert with Congress, will be responsible for determining the most appropriate approach.
Mobilizing resources and covering the additional costs of this initiative rests on four elements.
- Leverage existing U.S. bilateral investments. The 13 target countries were selected, in part, because they already feature ongoing U.S. investments in family planning, maternal and child survival, immunizations, and nutrition, along with HIV/AIDS, tuberculosis (TB), and/or malaria. A first step is to map how to build on current programs to prioritize outreach to adolescent girls and young women by detailing what programmatic capacities and resources can be tapped, and mapping U.S. country-level investments by program and site. The DREAMS partnership, funded through PEPFAR at an initial level of $385 million, is active in 6 of the 13 target countries, and could contribute to the program goals.17
- Leverage multilateral agencies, particularly in those areas where we are confident that greater U.S. commitments will bring other donor dollars to the table. At present, all 13 countries remain eligible for support from Gavi.18 As Gavi accelerates access to the HPV vaccine, the United States can contribute to this effort confident that other donors will help to cover the remaining costs.19 TThe World Bank’s Global Financing Facility has considerable potential to incentivize partner countries to invest International Development Association (IDA) resources.20 UN agencies, including UNICEF, UNAIDS, and UNFPA have a major role to play across most of these programmatic areas. The Global Fund, which invests in each of the 13 countries, can potentially further align its investments to more directly and reliably benefit adolescent girls and young women.
- Leverage industry and foundation partners. There are considerable opportunities to bring to scale select public-private partnerships— DREAMS; Pink Ribbon Red Ribbon; Saving Mothers, Giving Life—that are already hard at work in many of the activities recommended by the Task Force.
- Increase U.S. bilateral investments across all four programmatic areas (maternal and child health, family planning and reproductive health, nutrition, and immunizations). This will require careful sustained consultations with Congress, in the context of the overall changes the Trump administration will seek in the federal budget and within the constraints of the Budget Control Act.
“Confronting the challenges of adolescent girls and young women would leverage large gains in nearly every other field of health and economic development. It is impossible, for example, to take the next vital steps in HIV/AIDS prevention without empowering adolescent girls—helping them find more knowledge, skills, and influence over their own lives and futures. This has been, and should be, an entirely bipartisan matter. The Task Force report not only describes an urgent need, it provides a rigorous, detailed, costed-out policy framework to address that need. If the Trump administration pursues this type of initiative, it will find strong support across the ideological spectrum, including from critics on other matters. And such an initiative could unite members of Congress in an important shared mission at a time when unity of national purpose is all too rare. The implementation of these proposals would save the lives of countless mothers and newborns, reduce the risk of cervical cancer, and prevent many abortions. For myself, I regard this as a pro-life cause.” — Michael Gerson
Conclusion
We recognize that this proposed initiative is exceedingly ambitious and complex. Its launch by the Trump administration in concert with Congress could take a variety of forms under different scenarios. But whichever path is chosen to bring this initiative to life, it will require sustained high-level political will, matched by the support and good faith of the many other actors who will play critical roles. The sections that follow provide a deeper look at the four priority programmatic areas, governance and implementation, as well as extensive detail on costing and the selection of target countries

Photo credit: Salman Saeed
Summary of Goals and Costs
Overview: A signature initiative to accelerate progress on the health and wellbeing of adolescent girls and young women in 13 low-income countries where needs are greatest and U.S. investments are substantial.
TO DOWNLOAD THE FULL REPORT, CLICK HERE.